When there is nothing more to do…
Posted on February 29, 2016 9 Comments

It was early Sunday morning and our team had been up late the night before operating on a premature infant with an intestinal blockage. I am usually grateful when there is just one big problem to handle during a weekend of call, but that was not to be this weekend. At about 4:00 am, I was informed by the senior surgical resident that a woman with extensive burns had just arrived to Casualty (our ER). I briefly contemplated taking a shower, but instead prioritized coffee intake, then walked up the hill to the hospital. It was easy to find the patient…her burns extended onto her face which was not hidden by the white sheet which covered the rest of her body. The resident, Valentine, filled me in on the story: The woman lying in the bed was a mother to two young children who were playing inside of their house around an open fire. An open fire is a common enough occurrence in Kenya since it provides the means of cooking in most homes, but what evolved into an uncommon situation was that the two children began playing around the fire with a container of kerosene. Fortunately, the mother quickly recognized this and took the container from them. Unfortunately, the kerosene spilled onto her shirt, soaking it thoroughly which was then ignited by the fire. The fire was quickly extinguished, but not before burning the majority of the skin on her body. She travelled to a nearby hospital and then was sent on to Tenwek, now some 8 hours after her injury.
Together, our team examined her. She was completely awake and alert and was able to have a normal conversation with us. As expected, she was in some pain, but it was reasonably well controlled. Her burns were extensive…her back, chest, arms, and face were covered in second and third degree burns. In total, just over 60% of her skin was burned.
In the U.S., a patient with a 60% body surface area burn is a challenge…so much so that these patients are usually transferred to a specialized burn center to be cared for by burn specialists. Surviving a burn that involves 60% of the skin is possible in the U.S., but even with specialized care about half of these patients (depending on age) will ultimately die from their injury. In western Kenya, where there are no burn specialists and where hospitals are not equipped to take care of a patient of this complexity, the chance of survival is close to zero. And so, as we are assessing Mary, the extent of her burns and the reality that she will almost certainly die from these burns becomes clear.
As a missionary surgeon, I am charged with displaying Christ in both word and deed to my patients. The deed part comes naturally to us as surgeons. We like to fix things. We like using our hands and minds to correct a problem so that we can see a person healed. This paves the way for us to sometimes share, by word, who Christ is. Often times at Tenwek this is done by our Kenyan chaplaincy staff who can speak into spiritual matters with better cultural and language insights that I can. I am always grateful for our chaplains because, quite frankly, I am at times uncomfortable doing their job. I do not want the patient or family to think that the only way that I, the white guy, will provide care for them is if they agree to my religion. The reality is that there is an imbalance of power between us as physicians and our patients. We have knowledge, skills, ability, and resources that a desperate patient needs. Does my sharing of Christ in word coheres a patient? Possibly. Therefore, my approach is to display Christ primarily in deed by taking care of a patient’s physical needs. But on this morning, I have little to offer this patient this patient medically.
We explained to the patient and her family the extent of her injuries and the likely outcome. We give them the option of not doing any treatment, of just keeping her comfortable, but they refuse and ask us to do everything we can, to which we agree. We will need to intubate her- place a breathing tube- for which she will be sedated and communication will be difficult. Valentine, in Kiswahili, asked the patient about her faith. “Do you know Christ?” She does not, but after Valentine spends time telling her about who Christ is, she decides to give her life to him. We all pray together: the patient, her family, and our team. We prayed for healing and for comfort in the midst of a lot of pain. Tears flowed from her husband. After this we wheeled her to surgery…it was the last time she would talk to her family.
Skeptics might say that her faith was not genuine. They might say that she was scared for her life, or rather, her coming death. Some might even say we took advantage of this to achieve our own desires to “win people for Jesus.” However, the only place where we can fully see Christ is when we are stripped of everything. Only when we realize the frailties of our flesh, the briefness of this world, and the passing of material possessions can we truly see our need for the cross. And so, very likely, this lady came to know Christ in deeper ways than many of us who have followed Christ for years. But my role is not to be a judge. Instead, I am called to be a witness in a time of great need- a need that cannot always be met by modern medicine or years of training.
All things considered, our patient did well over the next 3 days. We worked hard to replace liter upon liter of fluid that she was losing because of her burns. She remained on a ventilator. We kept her pain controlled with IV pain medication. On what would have been her fourth day in the hospital, I arrived to ICU rounds to find her bed empty. She had died during the night.
Generally, as a missionary, I want to tell of stories of success, stories of great healing where God used me as his instrument to bring someone back from the brink of death. I want people to applaud the medical work that is done at Tenwek. This is a human mindset- and one that is self-glorifying. While there are truly amazing things that happen here, I have come to understand more completely that not all acts of healing are physical. Not all great interventions involve the use of sterile instruments and suture. For Mary, healing was achieved apart from these things.
A thrill of hope…the weary world rejoices!
Posted on December 31, 2015 9 Comments

As we sang Christmas carols at our Christmas Eve church service, a familiar and heart-wrenching wailing began in the background, coming from the direction of the hospital. We all know what this sound means…Someone has just lost a dearly loved one. You see, it is rarely a “silent night” at a hospital.
We have just celebrated our second Christmas season in Kenya. It has truly been filled with such joy! But amid the joyful celebrations and rewarding service opportunities, we are surrounded here by constant reminders that we still live in the “messy middle.” This term, “messy middle,” has been used by different people in different ways, sometimes to describe the timeframe between the starting and completion of a goal. But here, I mean the time between the arrival of Christ in human form as the promised redeemer of mankind…and His anticipated return to restore harmony, true PEACE, to His creation.
The struggles of this “messy middle” are not unique to Africa…they are just more intense here… more “in your face” so to speak. The pain of disease, illness, loss, grief…it touches us all at some point. In America, we tend to hide it away if possible. But in this place, a stone’s throw from a hospital in a region where most people live on less than two dollars a day, there is no hiding it. And so we hear wailing while singing carols. Or there’s the Christmas party, interrupted by an urgent request for blood donation for a patient undergoing emergent surgery after a trauma. And there were hundreds of families displaced on Christmas Day in a neighboring county, their homes burned down due to fires set from inter-tribal conflicts. And men with arrow wounds presenting to Tenwek from these same conflicts. And there are daily knocks on our door, asking for help due to these and other struggles. Life is messy.
So, yes, we celebrate Christmas with deeply grateful hearts…as this miraculous coming of Christ to earth gives us hope and promise of things made right and new…and we also longingly yearn for His rule as the true Prince of Peace. This promise gives us true JOY and HOPE even in the midst of pain and suffering. So we strive to LOVE as He taught us…seek PEACE where we can…DEFEND those with no defender…and build God’s kingdom here on earth until He comes to complete the task.
THANK YOU to all who gave toward my “Grown up Christmas list” and to those who give to our ministry year-round. You enabled us to love well this Christmas, and you blessed our community with your gifts. Since a picture is worth a thousand words, here are some pics that describe our Christmas:
We were able to “take” Christmas to one of the local orphanages, Kinduiwa home. It was a fun and humbling experience. We have such respect for the Kenyan pastor and his wife who are committed to the challenging task of raising these children in a safe and loving environment despite very limited resources.

The kids were thrilled to all receive new clothes!









This year we were thrilled to be on the giving side of Operation Christmas Child. After packing boxes in the US for years, this was very special! Tenwek Hospital received boxes to give all of the pediatric patients on Christmas Day.

Rees and Mary Taylor are helping prepare boxes for Christmas Day.

Heath had operated on this little boy earlier in the month, so it was special to be able to give him a box.






We had parties at the hospital, with fellow Kenya missionaries, and with the surgery residents. Below are pictures of our chief surgical residents as “living Christmas trees.” This is the closest we will get to a Living Christmas Tree in rural Kenya!

Dr. Damaris, a surgical chief resident, will be graduating in January

Dr. Blasto (yes, there’s a person under there!), also graduating in January
The girls and I continued our now annual tradition of homemade gingerbread houses (more like a village!). This is an anticipated event for the MKs at Tenwek, and one we have come to enjoy. I was much less intimidated this year by the lack of the “kit” and work involved to DIY!


Preparing to donate blood for an urgent need during one of our Christmas gatherings

Singing carols through the hospital

And just for fun…A Christmas tree topper you will only find in Africa!
“Truly He taught us to love one another; His law is LOVE and His gospel is PEACE. Chains shall he break, for the slave is our brother, and in His name all oppression shall cease. Sweet hymns of JOY in grateful chorus raise we; Let all within us PRAISE His holy name. Christ is the Lord! O praise His name forever! His power and glory evermore proclaim!” ~O Holy Night, verse 3

For online giving toward our ministry in East Africa, click here

My Grown Up Christmas List
Posted on November 13, 2015 Leave a Comment

Although there have been more recent releases, this song will always carry me back to the 1990’s and Amy Grant and a time when I thought I was much more grown-up than I really was! I am not as optimistic or naive as I was then, but now that I really am a grown-up, I do have a Christmas list that can’t be bought in stores. And these wishes don’t come from song lyrics, but from the backdrop of my daily life. Would you like to give a gift that really matters to someone this Christmas? If so, read on, because you can! …This is my grown up Christmas list:
1. Needed SURGICAL CARE for our poorest patients
Tenwek Hospital has become a referral center for the sickest and most complicated patients in the region. While our physician services are free through the support of our donor-team, the hospital operates by patient fees. The Tenwek Compassionate Surgical Fund lets us give free or discounted services to the most needy of our patients, and is critical in allowing us to offer quality care to the poor in our community. Most surgeries here can be covered with $400.

2. TEA PLANTS for our sustainable tea farming project
This sustainable project implemented with our national partners is designed to help support the daily needs of our local orphans. One acre of tea plants costs $250. Help plant fields of hope through the Tenwek Orphan Outreach Fund.


3. FOOD for our orphans
One 45 pound sack of corn costs $50. One 45 pound sack of rice costs $50. Each of these sacks can feed 50 children for 1 month! Invest in a healthy future for our community through the Tenwek Orphan Outreach Fund.

4. CLOTHES for our orphans
One pair of shoes costs $10. One school uniform costs $20. Invest in the practical needs of our kids through the Tenwek Orphan Outreach Fund

5. One year of EDUCATION for an orphan
Unfortunately schooling here is not free. One child’s preschool fees costs $75; One child’s elementary school fees costs $125; One child’s high school fees costs $500. Invest in opportunity through the Tenwek Orphan Scholarship Fund.

Thank you for considering a gift to support our Kenyan community in meaningful and lasting ways. Let us each seek to share the great great love of our Savior this season!
“For I was hungry and you gave me food, I was thirsty and you gave me drink, I was a stranger and you welcomed me, I was naked and you clothed me, I was sick and you visited me, I was in prison and you came to me… Truly, I say to you, as you did it to one of the least of these my brothers, you did it to me.” ~Matthew 25:36, 40

The Bygone Days of Summer
Posted on September 26, 2015 2 Comments

“Summer afternoon- summer afternoon; to me those have always been the two most beautiful words in the English language.” ~Henry James
I’m feeling a bit nostalgic today and thought I would reflect on our recent summer. I love summer. I have never been one of those moms who is ready for school to start. I love the late warm nights and slow lazy mornings of summer. I might live in an eternal summer if I could. For my past ten years of parenting, thoughts of summer have conjured words like sun, beach, peaches, cook-outs, cousins, grandma’s house, lake, camp. This year however, my summer memories hold words like goats, mud, and babies. Thankfully, it still also holds memories of cousins and beach and sun!
“Summer” in Kenya is very different. For starters, there isn’t really a seasonal summer. Being in the southern hemisphere, the months of June through August are actually our cooler months. Now “cool” is relative, as we almost always have sunny days with warm temperatures reaching near 80 degrees. In this way, our weather here is kind of like a perpetual enjoyable summer, without the sticky humidity of my US summers. So here, we define “summer” in terms of our break from school. And we did take a break from school. On our first day after finishing school, we greeted Heath’s sister and family for a visit. This started a summer of experiencing Kenya with and through a stream of visitors…family, friends, pastors, and short-term medical staff. We helped mud houses, colored and painted with orphans, held babies, took walks through the countryside, visited with Kenyan friends, and took safaris. We were so fortunate and blessed to be able to share bits and pieces of our lives here with friends, family, and visitors. I am thankful that we have memories with these special people in our new home. We hope that their visits here let them connect more with us in our new life, and even more so, than it will give a bigger and fuller and more real picture of God…as God of the universe and God of all people.

Amazing Kenyan ladies making the perfect mud.

Sabrina and I, attempting to “mud” a house.

This little guy is getting an early start on his mudding skills!

Goats are more fun than mud!

These girls were not afraid to get dirty!

More than 50 ladies fit into the small house to sing blessings and praises for the widow who received the house. Then we were gifted with congas and chai cups. I think we left the more blessed!

The trek back down the mountain was wet and slippery and deemed to treacherous for our “babies” by the Kenyan mamas…So they hoisted our kids onto their backs and carried them down. These women never cease to amaze me!

Bella getting a ride from a Kenyan mama.

The girls and their cousins helped feed a baby gazelle.

The kids explored the Kenyan plains on horseback…with hartebeest, gazelles, and zebra.

Nothing like starting the morning with a giraffe on your porch!

We loved introducing long-time friends to new friends.

These kids could have colored all day long!

Claire helping with water-paints, finding joy in the simple things.

The girls enjoyed showing their cousins their new “home.”

Rees holding a sweet little one at The AGC Baby Center (orphanage).

Claire and the girls loving on babies…

Mary Taylor loved making this little one laugh. Isn’t he precious?!

Claire was a big part of our spring and summer…In addition to serving in many ways, she filled the girls’ days with fun activities during August when I worked full-time. We look forward to seeing how God will use her in the world!

We took a short but wonderful family trip to the African coast before ending our “summer.”

Sisterly love and an amazing view!

Rees spent her entire 11th year in Kenya. We celebrated Kenyan-style!
I read a quote somewhere, “Some of the best memories are made in flip-flops.” I would have to agree, especially since in Kenya, flip-flops are year-round! (Although my girls might argue that the best memories are made in bare feet!) So even though our carefree days of no school and many visitors have ended for now, our flip-flop-memory-making days continue…

Can’t you tell that some serious memories were made in these flip-flops?!
Reaching Out
Posted on July 25, 2015 Leave a Comment
In previous posts and through other media forms I have tried to give a picture of the need for access to surgical care in rural Africa. Recently, this need was highlighted in a paper that was published in the Lancet and was subsequently reported on in the BBC. Please see this link to read more- No Access to Safe Surgery . The conclusion is that most of the world’s poor do not have access to adequate surgical care. This growing awareness of the worldwide surgial need has prompted brainstorming from various health organizations on how to meet this need. Certainly, training surgeons is one of the methods to help pave the way for better surgical care. This is what has drawn our family to Kenya. However, there are other ways. Surgical “camps” are one of the ways that various groups have used to try to relieve the surgical disease burden in one locality. The idea is to do as many surgeries as possible over a few days while providing this care for free or at a significantly reduced rate. Typically these camps are done in areas where there is not immediate access to to surgical facilities, and, often times, it is professionals from other countries who are coming to donate their time and expertise.

Brase Clinic in Migori, Kenya
Last week, I travelled to far western Kenya along with one of our third year residents, Dr. Valentine Mbithi, for a 3 day surgical camp. This well-organized camp is at a small clinic which is run by Kenya Reflief. At least monthly, teams (usually from the U.S.) come to do as many surgeries as possible over 3 days. However, for July, the team travelling from the U.S. was lacking surgeons… which of course is a key ingredient in providing surgery. We were asked to help fill the gap and we gladly accepted. I felt like this would be a great opportunity for Dr. Mbithi and I to participate in mission outreach, plus it would allow her to operate a little more independently as we would both be running OR rooms.

Inside the clinic, patients begin arriving for the day’s surgeries.

Our team setting up the OR on our first day.
We arrived on a Sunday afternoon after travelling about 3 hours from Tenwek to an area that I had not been before. The last hour was on a narrow road that twisted and turned through sugar cane farms. I felt grateful to arrive in one piece- we were run off the road twice by high speed buses who were out of control on the narrow roads. After settling in, we met the team who we would be serving with. There were four CRNA’s from various locations in the U.S., as well as a recovery room nurse. We quickly made our way to the screening clinic were we evaluated and scheduled patients for the next 3 days. The most common diagnosis was thyroid goiter. These huge goiters are often times caused by iodine deficiency and can grow so large that they cause problems with swallowing or even breathing. However, we also saw patients with hernias and other lumps and bumps. We worked into the evening, ate a big dinner, and then crashed.

Dr. Mbithi starting a hernia repair.
By 6:30 the next morning, we were back to the clinic and ready to start surgeries. We worked out of one OR which had two surgery tables, so Dr. Mbithi and I were in close proximity. If she had a question or concern, I could quickly provide guidance. In the morning we did smaller cases independently, and as the afternoon started, we began thyroid-fest. Our team was incredibly efficient. We had almost no break between surgeries, which as surgeons, we love. Thyroidectomies are more complex cases, so Dr. Mbithi and I would work togther during the key parts of the operations, and then one of us would close the wound while the other headed to the next table to start the next case. Our team worked until 9:00 or 10:00 at night for the next two days. In two and a half days of operating, we did 24 operations. In total, we removed 9 thyroids, fixed 5 hernias, and did several other smaller operations including a lip reconstruction from a poorly healed tramatic injury. We also performed the first cytoscopy (looking into the bladder with a camera) that had been done at the clinic.

Dr. Mbithi still smiling after a long couple of days of surgery
By Wednesday afternoon, we were beat. Our team members were incredible to work with and I give a big “hats-off” to Kenya Relief and the missionaries who are there on the ground making these camps happen. In addition to doing surgeries, we referred many patients who were too complex to operate on at the camp to follow up with us at Tenwek. In this manner, we were able to extend care and continuity that many short camps are unable to provide. As we drove home to Tenwek, Valentine asked me if we could bypass letting one of the other 13 residents come on the next trip so that she could return. This is what I am most thankful for… seeing our trainees develop a vision for service and outreach to those who are in desparate need.

Dr. Mbithi and I with the Kenya Relief team
Father to the Fatherless
Posted on June 22, 2015 1 Comment
“It’s such an honor,” we are told, “for wazugu (white people) to be invited do the final layer of the house.” We are preparing for “mudding” a house. Traditional houses here are fashioned from simple scaffolding made of sticks which are then filled in with several layers of mud. A local women’s ministry (Tabitha Ministry) works with village churches to help provide money for roofing supplies (rafters and a corrugated metal sheet) so that these simple houses can be built for widows and orphans who often find themselves without a home.
My nephews, Ryan and Eli, raised money for a house. Motivated by their upcoming trip to Kenya and wanting to contribute to our community here, they worked extra jobs around their school helping teachers clean and pack up their classrooms for summer break. They were able to earn almost $250, the amount needed to complete a house with roofing. Now, during their visit, we are going to help finish Betty’s house.
Betty, a 21-year-old orphan, has never had a house of her own. Her mother, Anna, spent much of her adult life doing anything she could to provide for her seven children…selling illegal brew and even her body. She rented rooms for her and her children in an area of town called “Satan’s Den.” In her last years of struggling with HIV/AIDS, Anna came to know Jesus. She grew in her faith through the Tabitha ministry’s Bible studies. She spread news of Jesus’ love throughout Satan’s Den, and began sharing Him with her children. Anna lost her battle with HIV/AIDS in 2010. Betty turned from God for a time in the aftermath of her mother’s death. Now, Betty is striving to follow Jesus and trying to create a home for her younger siblings.

Mixing up the “paint”
“The final layer is special,” we are told, “because it is a mixture of clay and animal dung, which provides a protective layer to the walls.” (Yes, animal dung…a nicer way of saying “cow poop”). So we scooped up large, dripping, smelling handfuls of the thick liquid and “painted” the walls with our hands. The ladies show us the proper technique…both hands, large sweeping motions, smoothing it into all the cracks. There’s no halfway effort to this. Doing it right means that the warm liquid runs down your arms, dripping onto your legs and toes. Throughout the day, as our “paint” mixture gets low, the ladies disappear and return with large buckets filled with fresh dung to replenish our supply. Nature’s supply shop…

Showing us the technique (always with a smile!)

Ryan working on the front wall of the house
Linda and Gladys finishing the outside

Eli wasn’t too sure about the “paint” but that didn’t stop him from helping!
A thicker gloppy mud is also made to fill in the space between the roof and the upper edge of the wall. This mixture is made by digging up dirt in a hole, adding water, then stomping on the mud until it is just the right consistency. Our kids all love this part!

Rees and Mary Taylor helping Peter prepare the mud for filling the gaps

Talk about dirty feet!
After finishing the inside and outside walls of the house, we wash up (in buckets because there is no running water) and share a meal in the new home with Betty and her family. Neighbors and friends keep squeezing into the freshly mudded room, unhindered by the flies or the odor. Scriptures were read and songs were sung…giving thanks to God for His provision and praying His blessings on the home. What a beautiful picture surrounded us of God providing through the body of Christ not just for Betty’s practical needs, but restoring hope and joy and family.

Betty with her siblings and Batiem (grandmother) outside of the finished home
Yesterday, while celebrating the admirable earthly fathers in my own life, I couldn’t help but think of Betty. I pray that she knows more strongly each day the love and security of our Heavenly Father who adopts us all as His own into His eternal family.
Rejoice before him – His name is the LORD.
A father to the fatherless, a defender of widows, is God in his holy dwelling. God sets the lonely in families, he leads out the prisoners with singing!
(Psalm 68:4-6)

“Let us pray for our mothers…”
Posted on May 12, 2015 Leave a Comment

“Let us pray for our Mothers… Because sometimes they die giving birth.”
This. A simple prayer request. Jolting in it’s content. But even more so because it was spoken by a 10-year-old boy, in his clear and crisp Kenyan-English accent, standing up bravely before a large church congregation.
It was our first Sunday to attend church at Tenwek after we arrived last fall. Inquiring later, I learned that this young boy is not an orphan, not motherless… Just a child growing up in a place where pregnancy holds as much risk as promise.
Many have asked me, “What about OB? How is your work?” I haven’t shared about my experiences in “Maternity” because, frankly, I don’t even know where to start. How is it possible that my previous and current worlds of obstetrics and gynecology even exist on the same planet? How did a trip across the ocean take me from a practice where I discussed with my patients the risks and benefits of epidurals, explained the evidence behind prenatal screening tests and childhood vaccines, reviewed the merits of personal birth plans, met with privately hired doulas, and even assisted in planning gender-reveal parties…to a place where the children in my community literally fear for the lives of their mothers.
I knew the statistics…I had shared maps and numbers and percentages with many of you in our days of preparations to help flesh out the “whys” that motivated our move to Africa.
Statistics like this:
- 800 women die EVERY DAY in the world due to pregnancy complications
- Almost 2/3 of these deaths are in Sub Saharan Africa
- The lifetime risk of dying due to pregnancy for a woman in Sub Saharan Africa is 100 times greater than for a woman in America (100 times!!!!)
And maps like this:

Cartogram of Maternal Mortality (Size of country is made larger or smaller based on maternal mortality)
But beyond the staggering statistics and dramatic maps are real people. These numbers now have names to me. Dorcas. Mercy. Nellie. Faith. Evelyn.

And they have families. Children left without a mother… sometimes newborns who I brought into the world on the brink of their mother’s departure from it.

Most maternal deaths are preventable, which makes the stark contrast between my two OB worlds even more difficult to reconcile. But too often, by the time mothers arrive to our facility, they have crossed a critical threshold beyond which our medical interventions have little chance of changing their outcome. Hemorrhage starting 24 hours prior to arrival with cardiovascular collapse already progressing too quickly. Infection setting in days ago, unrecognized or ignored, with septic shock already taking over. Advanced stage cancer, untreated, with severe malnutrition, in a body unable to withstand the strains of pregnancy any longer. Preeclampsia, unrecognized in a village clinic, with convulsions and loss of consciousness beginning several hours before arriving to our facility.
The reasons behind this unacceptably high death rate in mothers worldwide are complex and multi-faceted… Inadequate numbers of skilled health workers (trained nurses, midwives, or doctors), long distances to health care centers, poverty, cultural practices, and lack of information. Improving maternal health was 1 of the 8 Millennial Development Goals adopted by the international community in 2000. Improvements worldwide are being made. Maternal death rates are decreasing, but much too slowly to reach the proposed benchmarks by the goal of 2015. And there are still huge discrepancies between the rich and poor, and between those in urban and rural areas.
But my purpose here is not to fully expound on these reasons, or even to explore the many possible solutions, but rather to share about the beautiful and strong and brave women of my new home. They are remarkable…bearing incredible difficulties and sufferings with stoic grace. They love their children fiercely, dream expectantly, and persevere in amazing ways to care for their families. Their “barriers” to adequate health care are now the backdrop of my life. And it’s not OK.

Frustrated. Perplexed. Discouraged. Heartbroken. Indignant. These emotions co-exist within me on a regular basis in my new “normal.” In 9 years of private practice in America, I never lost a patient. Our team here lost 9 mothers in the month of January alone…4 more in February. And it’s not OK.
God does not ignore these strong and conflicting emotions. He has much to say about death and discouragement and earthly pain in His Word, because these elements surround us in this world if we are willing to see them. He uses words like “groan” and “burdened” and “grieved” and “afflicted” to describe our time on earth. But He also gives us the assurance that this is not how He intends for things to be. Yes, we protest against death with every fiber in our bodies; because we are created for eternity, not for these weak and temporary earthly bodies. And while I may not be able to save the life of every mother brought into my care, I am given promises to which to cling.
…Promise of death defeated… “He will swallow up death forever; and the Lord God will wipe away tears from all faces,” (Isaiah 25:8)
…Promise of light overcoming darkness… “The light shines in the darkness, and the darkness has not overcome it.” (John 1:5)
…Promise of GOD with us… “For it is God who works in you,” (Philippians 2:13)
…Promise of eternity… “But our citizenship is in heaven, and from it we await a Savior, the Lord Jesus Christ, who will transform our lowly body to be like his glorious body,” (Philippians 3:20)
So let us pray for our mothers, and for us all, that we not lose heart.
“So we do not lose heart. Though our outer self is wasting away, our inner self is being renewed day by day. For this light and momentary affliction is preparing us for an eternal weight of glory beyond all comparison, as we look not to the things that are seen but to the things that are unseen. For the things that are seen are transient, but the things that are unseen are eternal.” (2 Corinthians 4:16-18)

A Kenyan Christmas and a Happy New Year!
Posted on January 1, 2015 6 Comments

This year, our Christmas has been quite different from years past. While we have certainly missed family and familiar traditions, we are so grateful for the many new joys that God gave us here to make this season special. We thought we would share some pictures to give you an idea of our Kenyan Christmas…
We enjoyed hosting a Christmas party for the surgical residents.


The residents playing “reindeer games!”


This year our gingerbread houses had to be made from scratch. I think we have a new tradition!

The MKs made decorations for the pediatric ward at the hospital, then spread some Christmas cheer by decorating the ward.






One of the girls’ favorite times this season was Christmas carolling though the hospital wards. Instead of carolling, I was busy on call that night. These babies were serenaded moments after their birth.
Christmas carolling on Maternity
These babies are not relatives…just sharing a warmer (a regular occurrence here!).

I’m not sure that he liked the carolling!

We were grateful to have a visiting OB-GYN here to help over Christmas. Here she is teaching interns OB Ultrasound.
The kids packed 265 backpacks to give out at local orphanages. On Christmas Eve we were able to help host a Christmas party at one of these children’s homes and give out some of the backpacks. We all had so much fun celebrating with these sweet children!

Packing backpacks
The kids singing us a greeting

Helping the kids with Christmas crafts

They loved jumping rope!

Just some girl talk…

They jumped and jumped!

These girls just loved playing ball with Heath!

Don’t you love the joy on her face?!

No party is complete without cake!

These mamas LOVED the cake!

We presented the Christmas story through Jesse Tree ornaments, then decorated the “tree.”

The kids were so excited about the backpacks!
On Christmas Eve we worshipped at church, focusing on God’s gift in His son Jesus that gives us such cause to celebrate.

Candlelight service
On Christmas morning, we learned that “Santa” doesn’t just come from the North Pole…This year he came to us from Tennessee, North Carolina, Georgia, and Colorado! Who knew?!

Yes, she is really this excited over gum!
And anyone who knows MT knows how she is about stuffed animals!
We walked across the river to a friend’s house for chai (hot tea) and mandazis (a sweet fried bread), which is a traditional Kenyan Christmas treat.

MT and Cherono enjoying chai and mandazis

Pouring chai…Isn’t she a doll?!

Our girls were obsessed with the baby kittens!

Our sweet friend, who exudes the Joy of the Lord!
On Boxing Day (December 26th) we got to welcome some dear friends to Tenwek for a visit. Debbie and the Newman Family did pre-field training (MTI) together with us in May. It was wonderful to reconnect on this side of the ocean!

Taking a walk to the river

Happy to have another girl around!
Christmas hair!! So an interesting change takes place around these parts at Christmastime…all the girls and ladies get fancy hair-dos for Christmas! This especially transforms the little girls, who the rest of the year have super short hair (like at their scalp), but now have long pony tails and fancy styles. Rees begged for some Kenyan Christmas hair…so here she is!

Braiding took place on the front porch

Rees and her Christmas hair!
Living on the equator means sunshine and warm weather and lots of outdoor play, even at Christmastime!

Christmas break on the equator…sunscreen required
And last, but most certainly not least, I brought in the New Year by bringing this miracle baby into the world. She was delivered shortly after midnight in the ICU to a very sick mama who has a skeletal deformity of the chest causing severe pulmonary hypertension and respiratory distress. The decision was made to deliver this baby at 32 weeks gestation due to the mama’s worsening condition. At this state of prematurity, many babies here don’t survive (we don’t have ventilators designed for premature babies), but she came out crying and kicking and is doing great!
Happy New Year indeed!

Tenwek’s New Year baby
TOP TEN Differences in my daily life in Kenya
Posted on December 13, 2014 Leave a Comment
(By two MKs)
10. Sleeping under mosquito nets

9. Having pets (so far…a dog, rabbit, 2 hamsters, and an occasional chameleon)


8. Homeschooling
7. Getting mail and PACKAGES!!

6. Rarely driving anywhere (We walk to school, dukas (local shops), friends’ houses, etc.)

5. Animal on the roads (donkey, cows, sheep, goats, chickens, zebras, baboons, even lions if you’re on the Mara)

4. Friends readily available to play with…all day, every day!

3. Climbing trees

2. Going barefoot

1. Being together more as a family and eating lunch together every day!

One Night on Call…
Posted on October 27, 2014 12 Comments

I am sweating and my heart is racing. Twinges of panic appear but are then suppressed by thoughts: “How are we going to stop this bleeding?” “Where is it coming from?” “What happens if we can’t- I know the answer to that.” More twinges of panic. “Lord…help…” Blood fills the wound through a large crack in his skull. There are three of us working together: 2 residents and myself. I am supposed to be the experienced surgeon guiding the inexperienced through an operation that I have become confident doing through years of trial-by-fire. But I am not trained in neurosurgery and the brain seems a long way from the gallbladder right now. Bleeding continues. More sweating. We work together. One of us suctions, another elevates a fragment of bone away from the boy’s brain, and the other is ready with some packing to fill the hole to arrest the bleeding….
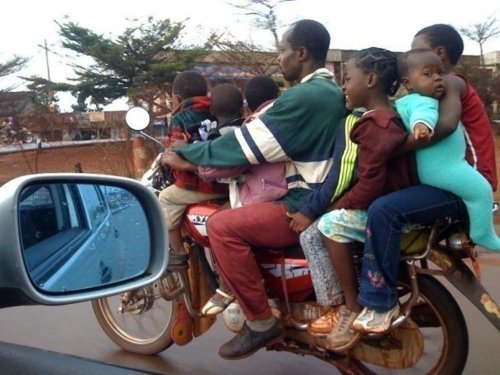
Several hours earlier, the young boy had been crossing the street when he was hit by a “boda-boda” or a “piki.” What we call a motorcycle. Motorcycles are a cheap form of transportation in a part of the world where the vast majority of people cannot afford a car. It is not uncommon to see 3, 4 or even 5 un-helmeted people on one motorcycle. But this child was just walking on the side of a congested street when he was struck. Following the accident his mother brought him to Tenwek where our team first evaluated him in “casualty”- the ER. He was 7 years old, but small for his age and had a big gash on his forehead. Fortunately he was awake and alert and it seemed that we would be able to just sew up his wound and get him home. But things changed. He started having seizures and became unresponsive to the point that we had to insert a breathing tube. Quickly he sent him for a CT scan which showed a depressed skull fracture with fragments of bone impinging upon his brain which was the likely source of his seizure. The fracture was located very close to a major blood vessel beneath the skull called the sagittal sinus. I would have rather avoided operating due to concerns of violating the wall of this vessel which can lead to heavy, difficult to control bleeding. But with his declining status, we did not have much of a choice so we proceeded to surgery…
With the packing, the bleeding has stopped for the moment. We gently lift additional bone fragments out of the wound and then wash out the dirt. There is a tear in his dura- the lining around the brain which contains the clear fluid that bathes the brain and spinal cord. With fine suture we carefully sew this up. I breathe a sigh of relief as it appears the bleeding has mostly stopped. A few fragments of bone are replaced like a jig-saw puzzle to fill the bony defect and then we closed his soft tissue and skin.
After taking him to the ICU still on a breathing machine, I walk home. It is late and I am having a hard time dodging mud puddles in the dark. The stars are out and it is a beautiful night. I am filled with contradictory emotion- I am grateful, I am relieved. But I am uncomfortable and humbled in this place where God has led me. I really want to sneak away to the airport, hop on a plane and fly back to the life I had. A life where I had most things figured out. But I know that that is not possible anymore. I am filled with passion for the work here- passion that could only come through grace. Passion that is impossible for me to generate on my own. Passion for the residents who are seeking to serve their people better. Passion for the patients who are enduring in the midst of incredible suffering
On rounds the next morning, the young boy is awake. He has already pulled his breathing tube out himself and he looks at me with an expression that says: “Dude, what was up with that breathing tube? And why do I have a killer headache?” He makes a great recovery and goes home a couple of days later. Have I simply failed to see God’s hand working in the past? Or is it only when I am stretched beyond my limits that I am able to see him working? Or is it that his strength is made perfect it my weakness? Likely all of the above.